
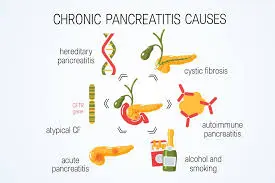
- Toxic-metabolic (alcohol/tobacco)
- Idiopathic
- Genetic (Trypsinogen gene mutations)
- Autoimmune
- Recurrent and severe acute pancreatitis
- Obstructive (divisum or tumor)
Pain: Abdominal pain is the most common and morbid symptom occurring in the majority of patients (90%) and is responsible for most hospital admissions related to CP. The pain is located in the epigastric area, often radiates to the back, is dull or boring in quality and worsens after eating
Endocrine insufficiency (diabetes mellitus): Endocrine insufficiency also occurs late in the disease. It is reported to the tune of 20–30% in various Indian studies. It can be controlled with diet, OHAs and insulin therapy.
Exocrine insufficiency: Pancreatic exocrine insufficiency may be mild, moderate or severe depending on the stage of the disease process, duration of disease and aetiology.
Typically, fatty diarrhoea (steatorrhea) does not become clinically apparent until 90 per cent of pancreatic function has been lost.

Various complications include pseudocysts, biliary or duodenal obstruction, internal or external pancreatic fistulae, left-sided portal hypertension and pancreatic malignancy.
Biochemical measurements:
Patients with chronic pancreatitis may have low, normal, or elevated levels of isoamylase, lipase, trypsin, and elastase.
It can be challenging to make a firm diagnosis of chronic pancreatitis in early or mild cases based solely on serum enzyme levels.
Radiological Examination:
Plain Abdominal Film: The plain abdominal film is typically the initial diagnostic procedure used to confirm the presence of chronic pancreatitis. As a positive finding, diffuse, specked calcification of the gland might be sufficient.
Trans abdominal ultrasound is a straightforward, non-invasive, and reasonably priced imaging method.
Large cavities (greater than 1 cm), calcification, and a dilated pancreatic duct (greater than 4 mm) are all signs of chronic pancreatitis (70 per cent sensitivity and 90 per cent specificity).
The following are the crucial components of managing a CP patient:
(1) Reduction of discomfort;
(2) Uphold nutrition and manage malnutrition
(3) Address complications.
Control of abdominal pain: The aim of therapy is to keep the patient’s pain under control, as complete pain relief is not anticipated.
The following techniques are employed to reduce the discomfort:
Analgesics: antioxidant enzymes in the pancreas.
Pregabalin Nerve Blocks: The two nerve block techniques used to prevent pancreatic pain afferents from signalling to the spinal cord are celiac plexus blockade (CPB) and celiac plexus neurolysis (CPN).
Endoscopic Therapy: The goal of endotherapy is to reduce ductal hypertension and relieve PD outflow obstruction in order to relieve pain.