


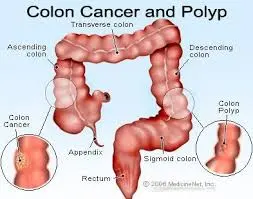

Colon cancer refers to cancer that develops in the colon, the longest part of the large intestine. Rectal cancer develops in the rectum, the final straight part of the large intestine that ends in the anus.
Risk factors:
- Aging: the risk of colorectal cancer increases as a person gets older.
- Lifestyle-related risk factors
- Diet: diet is the most important environmental risk factor for colorectal cancer. A diet that is high in red meat and processed meat, high in fat and/or low in fiber can increase the risk of developing colorectal cance
- High consumption of alcohol
- Obesity: overweight increases the risk of developing colorectal cancer
- Sedentary lifestyle
- Smoking
- Diabetes mellitus type 2 increases the risk of developing a tumour in the large intestine.
- Previous history of colorectal polyps
- Previous history of colorectal cancer
- Inflammatory bowel disease such as Crohn’s disease or ulcerative colitis
- Family history: approximately 20 % of colorectal cancers occur in a familial context
Symptoms
change in bowel habits, abdominal discomfort, fatigue, weight loss.Blood in stools could be a sign of alert. It could be visible to the naked eye or through a laboratory analysis of stools.
Investigations:
Colonoscopy
lighted tube is inserted through the anus into the intestine. It allows seeing the inside of the intestine. When a tumour is found within 15 cm from the anus it is considered rectal tumour, further away it is considered colon tumour.
CECT Abdomen and Pelvis for staging of disease
MRI Pelvis for staging of rectal cancer
PET CT in Advanced colorectal cancer
Tumour markers:CEA
Surgery
Surgery is the most usual treatment for colon cancer, especially if it has not developed. As for many cancers, surgery for colon cancer is most successful when done by a surgeon with a great deal of knowledge in the procedure.
Laparoscopic surgery
Laparoscopic surgery The word “laparoscopy” means to look inside the abdominal hole with a special camera or scope. To do a laparoscopy, between 3 and 6 small (5-10 mm) cuts are made in the stomach. The laparoscope and special laparoscopic tools are entered through these small holes. The surgeon is then guided by the laparoscope, which gives a picture of the intestinal organs on a video monitor.
Polypectomy
A colonoscopy, which is a large tube with a camera on the end, is entered into the rectum and guided to the polyp. A tiny, scissor-like device or wire loop removes the polyp.
Colectomy
The region of the colon where the cancer is, along with some healthy surrounding muscle, is removed. The associated lymph nodes are removed and looked at under a scope. Usually, the doctor then rejoins the sections of the colon. This operation also is called a hemicolectomy or partial colectomy.
Chemotherapy
Prolife offers the most up-to-date and effective chemotherapy choices for Colon cancer. Drugs are given by mouth or intravenously
Targeted therapy
Targeted therapy targets cancer’s specific genes, proteins, or the tissue conditions that add to cancer growth and survival. Targeted therapy blocks the increase and spread of cancer cells while restricting the damage to normal cells.
Radiation therapy
Radiation therapy uses strong energy sources, such as X-rays and protons, to kill cancer cells. It might be used to withdraw large cancer before an operation so that it can be removed more quickly.
When surgery isn’t an option, radiation therapy might be used to reduce signs, such as pain. Sometimes radiation is mixed with chemotherapy.