


- Heartburn: A burning sensation in the centre of the chest behind the breastbone, which has an upward moving quality toward the throat.
- Acid regurgitation: The awareness of acid or partially digested food from the stomach backing up into the esophagus, and occasionally into the throat and mouth.
- Other GERD symptoms may include:
- Difficulty swallowing
- Excessive burping or belching
- Sour or bitter taste in the mouth
- Chest pain
- Abdominal pain
- Nausea or gagging
- Cough, sore throat or hoarseness
- Obesity
- Pregnancy
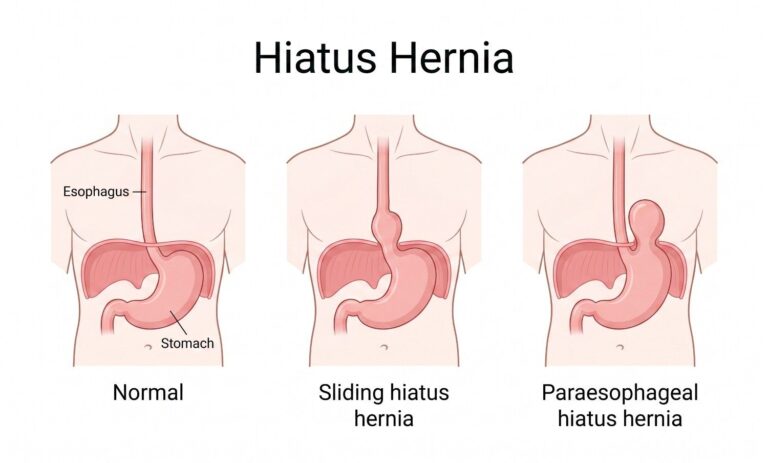
- Hiatus hernia
- Food choices
- Smoking
- Family history of GERD
Endoscopy: A thin, flexible tube (endoscope) with a light and a tiny camera is inserted into the oesophagus for this safe test.
Barium X-ray (upper GI series): The lining of the upper digestive tract is coated with barium so that it can be seen on an X-ray. 24-hour pH monitoring: In the oesophagus is a tiny tube (catheter) that has a pH sensor on it.
Over the course of a day, the sensor measures how acidic the oesophagus is, and the information is stored on a small computer that is worn around the waist for analysis in the future.
Esophageal motility study (EMS): In the oesophagus, a tiny tube (catheter) with a sensor is placed. The sensor used in this test gauges pressure and movement in the stomach and oesophagus to determine how well the LES is working.
- Avoid coffee, alcohol, fried or fatty foods, chocolate, peppermint, and other foods.
- Eat small, frequent meals as opposed to large ones.
- Before going to bed, wait three to four hours without eating or drinking anything.
- Using a foam wedge, raise the bed’s head or your upper body.
- attain and maintain a healthy weight
- Avoid smoking.
Medication
- Histamine H2-RAs, or H2-receptor antagonists, lessen the production of stomach acid.
- Stomach acid production is inhibited by proton pump inhibitors (PPIs). In addition to healing esophageal damage, this lessens heartburn symptoms.
- Agents that promote motility or prokinetics speed up the stomach’s emptying.
Indications for surgery include
- Ineffective medical management
- failure by the patient to comply
- excessive reflux,
- Endoscopy revealed severe esophagitis
- benign stricture resulting from ulcers or erosions
- the columnar-lined epithelium of Barrett (without severe dysplasia or carcinoma)
- being young and/or
- Patient decisions take into account the negative effects of ongoing medical treatment
Since GERD is a chronic condition, treatment must typically be continued long-term even after symptoms have been managed. Untreated GERD may occasionally cause significant esophageal damage.
Chronic scarring can cause the oesophagus to narrow (stricture), and repeated exposure to stomach acid can lead to the development of an esophageal ulcer and bleeding.
Barrett’s oesophagus, a condition that causes changes to the esophageal lining and raises the risk of esophageal cancer, may be present in some patients with long-term, uncontrolled GERD.
Since GERD is a chronic condition, treatment must typically be continued long-term even after symptoms have been managed. Untreated GERD may occasionally cause significant esophageal damage.
Chronic scarring can cause the oesophagus to narrow (stricture), and repeated exposure to stomach acid can lead to the development of an esophageal ulcer and bleeding.
Barrett’s oesophagus, a condition that causes changes to the esophageal lining and raises the risk of esophageal cancer, may be present in some patients with long-term, uncontrolled GERD.
Alarming symptoms are out of the ordinary for GERD and can point to more serious health issues.
Consult a doctor if you notice a change in your current symptoms or experience any of the following:
- Sudden weight loss
- Difficulty swallowing or a feeling that food is trapped in the chest
- Nausea / Vomiting
- Bloody stools (tarry black or red)
- Anemia

- Progressively having trouble swallowing solids and liquids (dysphagia)
- Unabsorbed food being regurgitated Reflux
- Pneumonia from aspiration
- Loss of weight (late finding)
- Chest pain (atypical finding)
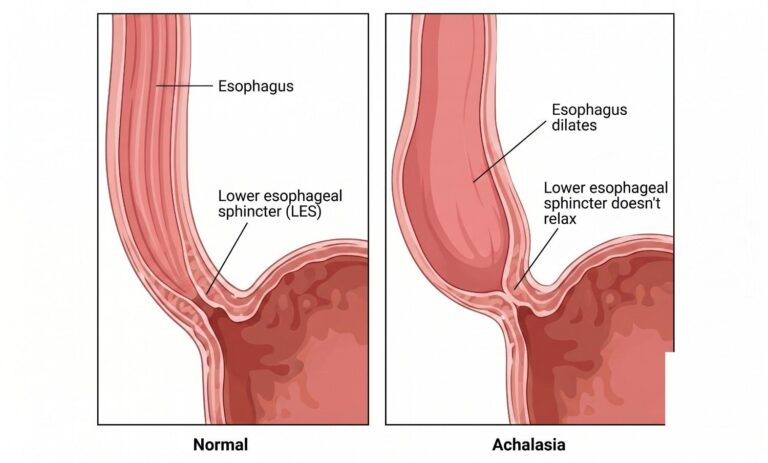
A patient with dysphagia to both solids and liquids and associated regurgitation of undigested food is typically suspected to have achalasia.
The following diagnostic techniques are frequently used in achalasia.
Endoscopy
Esophagogastroduodenoscopy (EGD) is usually necessary for patients who present with dysphagia in order to rule out a mechanical obstruction caused by cancer, which can mimic achalasia both clinically and manometrically.
Esophageal barium scan
The classic description of achalasia on a barium esophagram is esophageal dilation with a gradual taper down to the gastroesophageal junction giving a “bird’s beak” appearance. The objective measurement of esophageal emptying is the timed barium esophagogram (TBE).
Esophageal Manometry
It is the de facto method for achalasia diagnosis. Its purpose is to measure the pressures inside the esophageal along a flexible catheter’s length. Pressure data can be plotted as esophageal topography using high-resolution manometry.
Endoluminal Functional Lumen Imaging Probe (EndoFLIP)
EndoFLIP allows for the real-time measurement of gastroesophageal junction (GEJ) distensibility and operates on the impedance planimetry principle. The effectiveness of the treatment could be assessed using this parameter rather than LES pressure.
It cannot be cured but can be managed. There are five main types of treatment.
Pharmacotherapy
The least effective form of treatment for achalasia is thought to be oral pharmaceutical therapies. These drugs have an unfavourable side effect profile and a transient clinical response. The two drugs that are most frequently used are long-acting nitrates and calcium channel blockers.
Botox Injections
For patients who are unable to tolerate more invasive therapies like pneumatic dilatation or surgical myotomy, botulinum toxin is a helpful treatment option. The procedure entails evenly distributing up to 100 units of toxin with a sclero-needle just proximal to the squamo-columnar junction. The response rate is high during the first month of treatment, ranging from 80% to 90%, but the therapeutic effect quickly wears off over time, with only 50% of patients still experiencing symptoms after a year. Repeat treatments are therefore frequently needed every 6 to 12 months.
Pneumatic Dilation (PD)
The most successful non-operative treatment: 55-70% with a single dilation; >90% with multiple.
This causes the LES muscle fibres to be stretched and torn.
Most people need to receive treatment again after one dilation.
The rate of perforation is 1% (0.67–5.6%), and the overall complication rate is 11%. (Perforation, GERD, intramural hematoma).
Surgical myotomy, a procedure that divides the LES’s circular muscle fibres, was first carried out through an open thoracotomy and laparotomy.
But over time, less invasive procedures began to replace the outdated open approach. First, thoracoscopy was used instead of laparoscopic heller myotomy (LHM) due to its reduced morbidity and quicker recovery. LHM is now recognised as the gold standard for the surgical management of AC.
Esophagectomy
Conventional achalasia treatments frequently fail to control “end-stage” achalasia, which is characterised by a dilated and tortuous oesophagus (megaesophagus or sigmoid oesophagus). Before considering the more morbid esophagectomy, surgical myotomy should still be considered as the initial treatment even though PD is ineffective.
Peroral endoscopic myotomy: (POEM) is a cutting-edge endoscopic technique that myotomizes the LES using the oral cavity as a natural orifice entry point. By cutting only the inner, circular LES muscles through a submucosal tunnel made in the proximal esophageal mucosa, a surgeon performs the myotomy after tunnelling an endoscope down the oesophagus toward the esophageal gastric junction.
In contrast to laparoscopic surgery, which necessitates complete severance of the circular and longitudinal LES muscle layers, POEM does not involve this. To make it easier for food to enter the stomach, the dysfunctional muscle fibres that stop the LES from the opening are cut.
